
Feasibility and acceptability of a cohort study baseline data collection of device-measured physical behaviors and cardiometabolic health in Saudi Arabia: expanding the Prospective Physical Activity, Sitting and Sleep consortium (ProPASS) in the Middle East | BMC Public Health
 in the Middle East | BMC Public Health")
The study was approved by the Institutional Review Board at Princess Nourah Bint Abdul Rahman University, Riyadh, Saudi Arabia (IRB 22–0146), and was carried out in accordance with the principles of the Declaration of Helsinki.
Study design and procedures
Participants were informed about the study’s aims and asked to read and sign the consent form before any measurements were taken. After agreeing to participate, they were asked to attend two sessions at the Lifestyle and Health Research Center (LHRC) at the Health Sciences Research Center of Princess Nourah Bint Abdulrahman University. During the first visit, each participant’s anthropometric measurements (e.g., height, weight, waist circumference), blood pressure and heart rate, blood samples, and handgrip strength were measured. Next, the participants completed questionnaires on demographic information, dietary habits, self-rated health, self-reported smoking status, and the Global Physical Activity, Sedentary Behaviors, and Sleep behavior questionnaires. At the end of the first visit, the researcher attached the ActivPAL™ accelerometer device to their thigh which they were asked to wear for seven consecutive days. Participants were also provided with a diary to record their waking and sleeping hours [18]. On the 8th day of study, the participants were asked to attend the LHRC for session two where they returned the device and were interviewed (see Fig. 1).

Demonstration and summary of the study procedure
Participants and eligibility
The study aimed to recruit a total of 50 Saudi adults aged ≥ 30 years, which is generally considered a common sample size for feasibility studies [19, 20]. The eligibility criteria were: (1) Saudi nationals (2), resident in Riyadh, and (3) aged ≥ 30 years old. The exclusion criteria were: (1) having a current medical condition that forces them to be chair-bound or bedridden for more than half of their waking hours (2), being allergic to plasters or adhesives (3), being allergic to low-density polyethylene (4), having a skin condition that would prevent them from wearing the monitor, and (5) those who may need to pass through a metal detector/security checkpoint during the duration of the study. The study’s aims, protocol, and procedures were clearly described to all participants before any measurements were taken.
Recruitment
Participant recruitment was carried out over the month of November 2022. Participants were recruited from different locations across Riyadh, Saudi Arabia, by using electronic flyers on social media (e.g., Twitter, WhatsApp) that provided information about the study and the researcher’s contact details. Prospective participants who were interested in joining the study were asked to provide their contact information via a link to Google Forms featured in the study description. The participants who initially expressed interest but later decided not to join were invited to share their reasons for non-participation through a physical or telephonic meeting.
Measurements based on ProPASS methodology
The current study employed the ProPASS method and protocol for new cohort studies that seek to join ProPASS prospectively [14, 21]. All measurements were taken by researchers that were well-trained in the ProPASS protocol and methods. Blood pressure and hand grip strength measurements were taken three times, and the mean average was then calculated; all other measurements were taken only once.
Anthropometric measurements
Height (to the nearest 0.1 cm) and weight (to the nearest 0.1 kg) were measured with a stadiometer (SECA 284; Seca, Hamburg, Germany), and scale (SECA 284; Seca, Hamburg, Germany), respectively. Waist circumference (to the nearest 0.1 cm) was measured midway between the lower rib margin and the iliac crest at the end of a gentle expiration [22]. Body mass index (BMI) was calculated using the standard calculation (height in meters squared/body weight in kilograms).
Blood pressure and heart rate
Blood pressure was taken after resting for five minutes in a sitting position. Blood pressure was taken three times with one minute between measurements and the average reading was recorded [23]. Blood pressure and heart rate were measured using a Welch Allyn Connex 7300 Spot Vital Signs Monitor, which provides a high degree of accuracy [24]. Mean arterial pressure (MAP) was then calculated (MAP = 1/3 * SBP + 2/3 * DBP in mm Hg) using the average of both the SBP and DBP values [25].
Blood samples
Non-fasting finger-prick (capillary) blood samples (40 µL) were collected for analysis after warming the finger for five minutes. A drop of blood was taken directly from the heated finger to be analysed for blood glucose, triglycerides, total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol. A previously validated CardioChek PA analyser (CardioChek PA Blood Analyser, UK) was used to analyse the blood samples [26, 27].
Medication use
Participants’ medication use was evaluated by the question: Do you currently use any prescription medicines? If the answer was yes, the participants were asked which medications they use, such as medication for high blood pressure, high cholesterol, asthma, COPD, anxiety, depression, thyroid problems, allergies. They were also asked whether the medication was in the form of tablets, or nasal sprays, whether the medication was anti-inflammatory, chemotherapeutic, urological, birth control, or neurological, and the age at which the participants had begun using the medication.
Familial disease history
Familial disease history was assessed by the question: Do your parents, siblings or children have, or have they ever had, some of the following diseases before the age of 60? The responses included asthma, hay fever/nasal allergies, chronic bronchitis, emphysema or COPD, anxiety or depression, myocardial infarction (heart attack), diabetes, stroke or brain hemorrhage, and cancer. The responses were yes, no, and I don’t know.
Chronic health status
Participants’ chronic disease status and/or long-term health issues were assessed by the question: Have you had, or do you have any of the following diseases? The responses included angina, myocardial infarction (heart attack), heart failure, peripheral vascular disease, atrial fibrillation, stroke/brain hemorrhage, thrombosis, pulmonary embolism, asthma, COPD or emphysema, diabetes, hypothyroidism (low metabolism), hyperthyroidism (high metabolism), cancer, migraine, psoriasis, kidney disease, arthritis (rheumatoid arthritis), Bechterew’s disease, gout, mental health problems, osteoporosis, sleep apnea, arthrosis, nerve disease, hearing/ear disease, eye disease, and infection. Those who replied yes were asked a follow-up question: How old were you when you had it for the first time?
Mobility limitations
The questionnaire was based on three questions on performance-based measures of mobility, which had already been translated and culturally adapted into Arabic [28]. These three questions are valid and reliable tools to identify the early indications of disability and can be used as indicators to identify those at high risk of future disability [29]. Self-reported mobility was assessed via the following questions: (1) Do you have difficulty in walking 2.0 km? (2) Do you have difficulty in walking 0.5 km? and (3) Do you have difficulty in walking up one flight of stairs? The five response options were: (1) able to manage without difficulty (2), able to manage with some difficulty (3), able to manage with a great deal of difficulty (4), able to manage only with the help of another person, and (5) unable to manage even with help.
Dietary habits
The dietary habits questionnaire was translated and culturally adapted into Arabic [28]. The questionnaire assessed the dietary habits of the participants was adapted from the Survey of Health, Aging, and Retirement in Europe (SHARE), which has been demonstrated to be a valid and reliable tool for assessing diet [30]. The questionnaire focused on the consumption of dairy products, legumes, eggs, meat, fruit and vegetables.
Self-rated health
A set of valid and reliable questions adapted from Idler et al.’s (1997) questionnaire was used to assess participants’ self-rated health by asking them to rate their health status using the following questions: (1) In general, would you say your health is…: Excellent; Very good; Good; Fair; Poor; (2) Compared to one year ago, how would you rate your health in general now?: Much better now than one year ago; Somewhat better now than one year ago; About the same; Somewhat worse now than one year ago; Much worse now than one year ago [31, 32].
Smoking habits
Self-report questions on smoking behavior were adapted from the UK Biobank questionnaire and were used to assess participants’ present and past smoking habits including at what age they began smoking. the number of cigarettes smoked per day, the type of tobacco used, the duration of smoking, and, among former smokers, the age when smoking ceased [33].
Physical behaviours
Physical behaviors such as physical activity, sedentary behavior, and sleep were measured by using (1) self-reported and (2) device-based measures:
Self-report measures
Physical activity was measured on a self-report basis via the Global Physical Activity Questionnaire (GPAQ) which was translated into Arabic and previously validated [34]. In addition, the Sedentary Behavior Questionnaire (SBQ), which had already been translated into Arabic [28], was used to subjectively assess participants’ sedentary behavior time [35]. Lastly, the Pittsburgh Sleep Quality Index was used to assess sleep quality and sleep disturbances over a one-month period [36].
Device-based measures
Physical behaviors were measured by wearing a thigh-worn accelerometer device (an ActivPAL™ Micro4, PAL technologies, Glasgow, Scotland) that participants wore continuously for 24 h for seven full days [37]. The Activpal™ device was sealed with a nitrile sleeve and attached with a medical waterproof 3 M Tegaderm transparent dressing on the front of the right mid-thigh on the muscle belly by a well-trained member of researcher team. The ActivPAL™ monitor is a valid and reliable measure of time spent walking [38], sitting, and standing time in healthy adults [39]. In addition, the participants were asked to fill in a recording sheet that included a sleep diary (times that the participant went to and got out of bed), as well as, the dates and times when the accelerometer fell off or was removed.
Physical function
Physical function was objectively measured using a digital hand-grip strength dynamometer (Takei Hand Grip Dynamometer 5401-C, Japan) via three successive hand-grip assessments for each hand (left and right); the mean value for each hand was then recorded. The instrument can measure hand-grip values from 5 to 100 kg; the minimum unit of measurement is 0.1 kg. The tool is a good health outcomes predictor [40, 41].
Data collection evaluation of feasibility
Overall, the study evaluated feasibility in two main stages where feedback from the first six participants was used to resolve any unforeseen issues in the protocol implementation on the remaining participants. Any changes to the procedure were documented.
The current study evaluated the feasibility of Saudi adults’ participation based on the following constructs: (1) recruitment capability (2), acceptability and suitability of study procedures, and (3) resources and ability to manage and implement the study. Table 1 outlines the feasibility constructs, measures, outcome definitions, and methods employed. In evaluating feasibility, the current study followed the recommendations for a feasibility study as reported by Orsmond and Cohn, 2015 [42].
Overall, the study collected data on the feasibility constructs via tracking the registration, equipment availability, and time spent on various tasks performed (for example training researchers, performing various tasks like attaching the sensor) and completion rate (such as tracking diary entries, questionnaire entries and number of days with accelerometer data), via personal contacts (for information on barriers and facilitators of participation), via processing sensor data, and via interviews after the measurement (for example obtaining information on potential issues during measurement and willingness to participate).
Participant interviews after measurement
After the completion of the study, face-to-face semi-structured interviews were conducted with all participants who had completed the 7-day study period. The aim of these interviews was to collect comprehensive feedback regarding participants’ experiences with the study protocol, with the goal of capturing additional insights that was not captured by other feasibility measures. Some examples of such measures were motivations for joining the study, their expectations prior to participation, and their levels of satisfaction with the study procedures. A detailed interview guide is described in Appendix A [28, 43, 44].
Statistical analysis
Descriptive analysis summarized participants’ demographics, anthropometric measurements, health status, clinical measurements, physical behaviors characteristics, and interview questions responses. The continuous variables were characterized using mean ± standard deviations (SD), while categorical variables were presented using frequencies accompanied by percentages (%). The recruitment rate was calculated by the number of participants who participated and signed the consent form / total number of participants who registered in the study (see Fig. 2). Additional analyses were performed to compare participants who reported burden with those who reported no burden of participation (see supplementary materials). T-tests and Chi-square tests were employed for this comparison. IBM’s Statistical Package for the Social Sciences (SPSS) (version 27 SPSS, Inc. Chicago, Illinois) was used to conduct the qualitative analysis. The raw data of ActivPAL were analyzed by using the ActiPASS software (ActiPASS © 2021 – Uppsala University, Sweden).
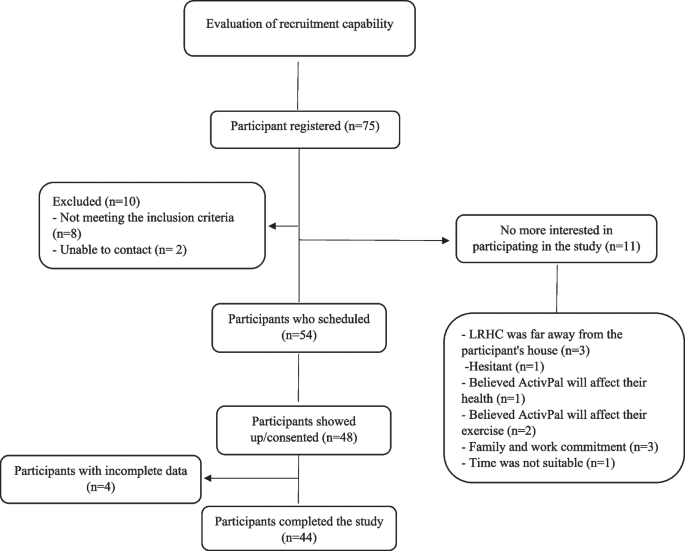
Recruitment and study participant’s diagram
link


:max_bytes(150000):strip_icc()/A-Physical-Therapist-Shares-the-Most-Underrated-Physical-Activity-94666d193c98412ca90ffbcc23339f90.jpg "Experts Say This Exercise Is the Most Underrated")



