
Effects of household air pollution and healthy lifestyle associated with gestational diabetes mellitus

Study setting
This is a prospective birth cohort study in Zunyi, Guizhou Province, China, based on the National Key Research and Development Program “Environment and Embryonic Development.” Pregnant women from Xishui County, Meitan County, Zunyi Medical University Hospital, and the Second Affiliated Hospital of Zunyi Medical University in Zunyi City, China, were surveyed using questionnaires, and their pregnancy outcomes were followed up. Pregnancy outcomes, data, and specimens were collected between 2019 and 2022. The baseline, exposure, and follow-up data were combined and organized into a database for the Zunyi birth cohort, including 6853 pregnant women.
Study participants
The cohort included pregnant women aged 20–45 years with a gestational age of 0–13 weeks, spontaneous conception, and singleton pregnancies. The exclusion criteria were severe chronic and infectious diseases, such as cancer, which can lead to cardiovascular disease, chronic renal failure, and HIV infection. Information on general demographics, home and work environments, lifestyle, and dietary and nutrient supplementation was collected through questionnaires at two visits during pregnancy (at recruitment) and postpartum. This study was performed in accordance with the principles of the Declaration of Helsinki. The protocol was approved by the Ethics Committee of Zunyi Medical University (No. [2019] H-005), and each participating pregnant woman voluntarily signed an informed consent form.
The study screened 6,583 participants in the baseline survey (2019–2022), excluding those with a previous history of diabetes (n = 93), home energy deficiency (n = 102), and lifestyle deficiency (n = 124). Pregnancy was classified according to the time of the pregnant woman’s last menstrual period, which was divided into the spring, summer, fall, and winter seasons. Owing to the consideration that if the pregnancy season was in the spring, the use of fuel for home heating was in the later stages of pregnancy, pregnant women with spring pregnancies (n = 1926) were excluded, with a total of 4338 participants included, as detailed in Fig. 1.
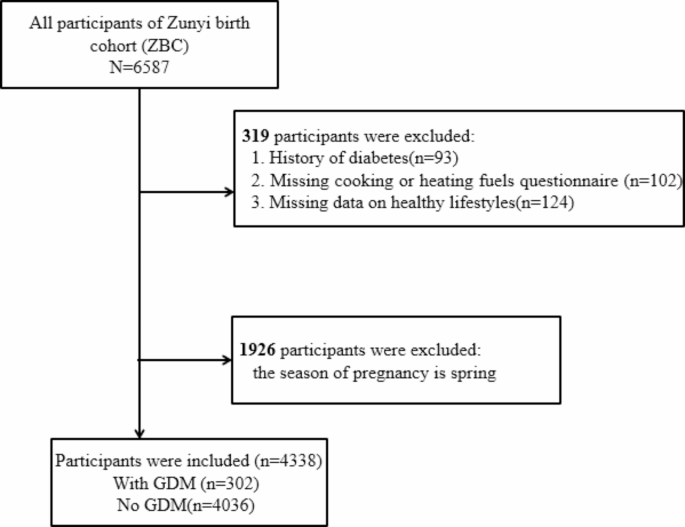
Flow chart of the study participant selection process.
Household air pollution
Information on household air pollution was collected through the interview questionnaire. The questionnaire contained the questions, “Which fuel is mainly used for cooking in the household during pregnancy so far?” (wood, coal, induction, or natural gas [liquefied petroleum gas/natural gas/biogas]) to assess the use of the main cooking fuel in the household, “How many times a week do you cook during pregnancy?” to assess the frequency of cooking during pregnancy, and “Is exhaust equipment such as hoods, exhaust fans, etc. installed in the kitchen?” to assess kitchen ventilation.
The questionnaire contained the questions, “What are the measures for heating in winter (central heating, coal-fired stoves, natural gas, electricity, or wood)?” to assess the use of fuel for home heating and “whether air purifiers are used in the rooms.”
Fuels are divided into clean fuels and solid fuels according to their impact on air pollution21. Household fuels are those used cooking and heating. Solid fuel is defined as coal, wood/straw fuel, and kerosene; clean fuels is defined natural gas, liquefied petroleum gas, and electricity. This study defined home pollution exposure as participants who used solid fuels and those who used clean fuels as controls.
Gestational diabetes mellitus
GDM was identified in the study participants by performing a 75-g oral glucose tolerance test between 24 and 28 weeks of pregnancy, with the diagnostic criteria being ≥ 5.6 mmol/L fasting, ≥ 10.3 mmol/L 1 h after glucose administration, and ≥ 8.6 mmol/L 2 h after glucose administration, with two or more of the results reaching or exceeding the normal values and the diagnosis of GDM being made. The diagnosis of GDM was confirmed by the attending physician and their supervisor at the respective hospitals, i.e., the First Affiliated Hospital of Zunyi Medical University, the Second Affiliated Hospital of Zunyi Medical University, Xishui County People’s Hospital, and Meitan County People’s Hospital.
Healthy lifestyle score
Based on a literature review on factors influencing lifestyle habits related to GDM, this study analyzed five lifestyle habits related to gestational diabetes12,13,14,15,16,17,18,19,20: physical activity, body mass index (BMI), dietary status, sleep, and vitamin D supplementation.
Physical activity status was determined by asking about the frequency, mode, and duration of participation in physical activity from the first 6 months of the current pregnancy, and participants who exercised ≥ three times per week with moderate intensity were considered to be engaged in high-quality physical activity. Since the number of pregnant women who could meet this standard of healthy exercise in this study was very low, and there was no association between healthy exercisers and GDM, this factor was excluded from the analysis. Participants were defined as healthy eaters if they consumed vegetables and fruit > 5 days per week. This categorization was accomplished by collecting the frequency of vegetable and fruit consumption from the year prior to the baseline survey to the current stage of pregnancy, rather than distinguishing between high and low intakes of vegetables and fruits by portion size22. Sleep status was associated with the length of sleep per night, defining ≥ 7 h as a healthy sleeper23. The vitamin D supplementation status defined pregnant women who were supplemented with vitamin D during pregnancy as nutritionally healthy24. According to Chinese standards, a pre-pregnancy BMI of less than 24 is considered a healthy body type25.
Diet, sleep, BMI, and vitamin D supplementation data were included in the final analysis of healthy lifestyle factors. One point was scored for each criterion met, or zero if unmet. Scores ranged from 0 to 4; higher scores indicated a healthier lifestyle. Subsequently, we categorized the participants into three modifiable risk categories (low, 0–1; medium, 2; and high, 3–4 scores). Referring to previous literature on criteria for scoring healthy lifestyles, having 3 or more healthy styles at the same time was defined as having good lifestyle habits26.
Covariates
Covariates were selected based on the baseline profile data. The pre-selected, potentially relevant covariates and confounding variables were based on previous literature regarding associations with GDM27,28,29.These included age (continuous; 24, 25–29, 30–34, and 35 years), marital status (married/cohabiting and unmarried/divorced/widowed), occupation (employed, farmer, and others), education (middle school or below, high school, and college or above), smoking status (yes or no), Passsive smoking status (no, sometimes, frequent), alcohol consumption (yes or no), and season of pregnancy (summer, autumn, or winter).
Statistical analysis
Continuous variables were described by means and standard deviations (SDs), and categorical variables were described by the number of cases and proportions. Continuous variables were described by t-tests and categorical variables by chi-squared tests. Multifactorial logistic regression was performed to evaluate the association between different types of household air pollution, lifestyle factors, and GDM. We adjusted for confounders to estimate the GDM risk ratio with a 95% confidence interval (CI). Additionally, we assessed the association between healthy lifestyle habits and GDM. Household use of solid fuels for heating and cooking was analyzed separately in relation to the prevalence of GDM, and the effect of combined exposure to two solid fuels or exposure to only one solid fuel was compared with that of two clean fuels. Healthy lifestyle scores were analyzed as continuous categorical variables. For categorical analyses, we compared the risk of GDM in the medium and high subgroups, using the low subgroup as a reference (only one or no healthy lifestyle factors). We adjusted for potential confounders, including age, marital status, occupation, literacy, smoking, alcohol consumption, and season of pregnancy.
We explored the extent to which a healthy lifestyle influenced the role of household air pollution on GDM by testing for potential modifying effects. First, the trend effects of a healthy lifestyle and GDM were calculated for two different heating fuel scenarios, followed by an analysis of the relationship between healthy lifestyle scores and GDM under the stratification of home heating fuel type. Finally, the additive interaction indices between solid fuels for home heating and healthy lifestyle scores (categories) were analyzed, and the relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (SI) were evaluated using logistic regression models. RERI > 0, AP > 0, and SI > 1 denote positive additive interactions, while RERI < 0, AP < 0, and SI < 1 indicate negative additive interactions. Additive interactions were statistically significant when the 95% CI for RERI or AP did not include 0 or when the 95% CI for SI did not include 1. Finally, to test the stability of our results, we evaluated their robustness using stratification and sensitivity analyses. First, we weighted the healthy lifestyle scores based on the beta coefficient of each lifestyle factor in the logistic regression model. Then, we excluded women with gestational hypertension, and history of parents with diabetes. Data were inputted and examined utilizing SPSS 22.0 software, and statistical analysis was carried out through SPSS 22.0 and R version 3.4.0. Statistical significance was established as a p-value blow 0.05 (two-tailed).
link

:max_bytes(150000):strip_icc()/A-Cardiologist-Shares-the-Most-Meaningful-Change-You-Can-Make-for-Better-Heart-Health-e058d2d7f85a41ffa03cd0692f08e0de.jpg "Limit This Food for Better Heart Health")




